
Burnout In Surgeons: It’s Not A Resilience Problem
You can't yoga your way out of a system that's built on your back
Burnt Out? Stuck? You're Not Broken
–
Find Your Discernment
–
Click Here To Work With Me
–
Burnt Out? Stuck? You're Not Broken – Find Your Discernment – Click Here To Work With Me –
In 2021 alone, 117,000 physicians left the U.S. workforce.
To put that into perspective, that’s the equivalent of four and a half years of graduating medical school classes, all walking away from medicine in a single year. It’s not just doctors, either. Three hundred thousand nurses left the profession in the first two years of the Covid pandemic.
The pandemic didn’t create the healthcare burnout epidemic, but it did expose it. It exposed what we all knew: burnout is a massive problem in healthcare, and it’s been building in this profession for decades.
And, in a way they really haven’t before or since, health professionals during the peak of the pandemic voted with their feet. But now that the acute phase of the pandemic is over, we’re doing less voting with our feet—all while the burnout has, if anything, gotten worse.
The system tells us that it’s because we’re not resilient enough. We need to double down, keep our heads down, and work through our burnout, all with the help of resilience training and wellness courses.
Which we know don’t work. Because burnout isn’t a resilience problem.
Treating burnout with wellness courses and resilience training is like treating an infection with the wrong antibiotic and then wondering why the patient became septic.
PS. Have you hit that inevitable burnout wall in your own surgical career? Let’s talk
Precocious Identity Formation Drives Surgeon Burnout
If burnout isn’t a resilience problem, then what is it?
Let me answer that by introducing you to a client of mine named Janet.
Janet’s not her real name. I’ve changed her name and some identifying details, but her story is intact.
Janet is a surgeon who staffs a surgical ICU at a big academic hospital on the east coast.
And she has known, since the age of six, that she wanted to be a doctor.
Both of Janet’s parents were doctors. Although she had a fraught relationship with her dad, and, conversely, a relationship with her mom that bordered on hero worship, both parents steeped Janet’s childhood in stories that lionized the profession of medicine.
By the age of twelve, Janet was able to articulate everything she wanted in her life: she wanted to be the person that others would call in an emergency. When she walked into a patients room, she wanted people’s shoulders to drop. “Whew…Janet’s here. We’re going to be okay.”
She pursued this goal with a single-minded devotion—through college, medical school, a surgical residency, an ICU fellowship, and her attending years.
And then Covid hit and, like so many of us, she burnt out. But, also like so many of us, because Janet had invested so much into her training, because she had finally become the person she’d always dreamed of being, and because her patients needed her, she had no choice. She did what she knew how to do: she put her head down, showed up, day in and day out, despite the burnout.
The collateral damage included her stomach lining and her marriage, both of which deteriorated in 2021.
What is burnout? How does it show up, especially in surgeons?
There are three strands in Janet’s story that I want to unpick, three legs to the surgical burnout stool.
The Three Legs of the Surgeon Burnout Stool
Leg One: Medicine As An Identity
Janet’s story is not unusual. About 73% of physicians know before age twenty that they want to practice medicine. And nearly a third decide before they even reach their teens.
Think about that for a second.
Before our prefrontal cortexes are even a glimmer in our midbrains’ eyes, we’re telling everyone that we’re going to be doctors.
And even if we’re in the 27% of doctors who decide after adolescence, our medical training is structured in such a way that decisions we make in our mid-20s—like what specialty we’re going into—must necessarily follow us for the rest of our professional lives.
Layer onto this precocious identity formation the sheer weight of the emotional investment into becoming a surgeon. The researchers Anders Ericsson and Robert Pool, who study expertise, describe three escalating levels of practice, all of which are necessary to become an expert.
The first, naïve practice, is simple rote repetition. This is tying surgical knots. How many of us, as third-year medical students, were handed a packet of 2-0 silk ties and told to throw as many knots as we could on every vertical surface in our apartments? That’s naïve practice. Super important, but not, alone, sufficient.
Then there’s purposeful practice, practice paired with meta-evaluation. Purposeful practice broadens our comfort zones. The skills we learn at one level become the baseline for the next set of skills.
And finally, there’s deliberative practice. This is full commitment practice, the apprenticeship-style all-in investment that turns medical students into surgeons.
Each rung on this echelon of practice demands ever greater emotional investment, and each one reshapes how we think. The more we invest, the more invested we become.
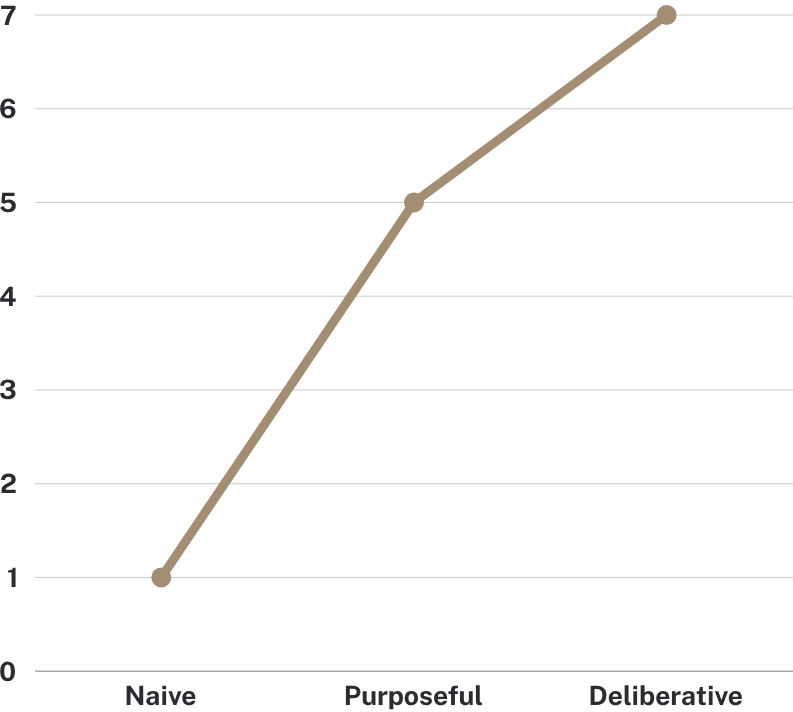
The more intense the practice, the higher the emotional investment it requires
In other words, medicine stops being something you do. It becomes something you are.
The data make this explicit. In a 2025 survey, only 12% of physicians said they would recommend a career in medicine to a young person. Meanwhile, in a different survey from the same year, 32% said they would choose the career again themselves.
In other words, nine in ten doctors won’t recommend the path of medicine, while a third would still walk it themselves.
That gap is identity. It’s the fact that we don’t work in medicine. We are doctors.
Leg Two: We Change
In his absolutely brilliant book, Falling Upward, the Catholic priest Richard Rohr argues that adult life has two halves.
In the first half of our adulthood, our focus is achievement. Now, what we achieve varies. For some of us, achievement is money; for others it’s recognition. It may be impact, it may be doing good in the world, it may be academic advancement.
But whatever it is, Rohr says that the first half of our lives is about building our ego structures through achievement.
And then something shifts. Something inchoate and inexorable happens to our inner worlds, such that, in the second half of our lives, we move toward what Rohr calls the “village elder” stage. The metrics that drove us, the things that were important to us at twenty-six, slowly lose their grip.
The German psychologist Erik Erikson agreed. Seventy years ago, he proposed a framework of psychosocial development that supports a similar arc. In this framework (which has been around long enough to have research to support it and research to contradict it), humans walk through eight developmental stages, at the center of which is a singular tension to manage. If we manage that tension well, then we move on to the next stage prepared for its tension.
If we don’t, future stages become even harder.
Erikson called the central tension in late adulthood generativity versus stagnation. In other words, do we continue pursuing the same achievements that built our identity decades ago—a choice that leads to stagnation and stuckness?
Or do we realign our work with the person we’ve become? Do we continue toward generativity?
The crux of the “midlife crisis” is here: What drove us at 26 no longer drives us at 46. We have changed inside and we crave an outside that matches.
I hear this sort of story so often from clients. They spend twenty years working toward the full professorship, the successful private practice, the national academy membership, only to arrive there and realize that it now feels empty. That’s because the person who set that goal at twenty-six has become someone else by the time the goal is reached.
We change.
Don’t stay stuck in decision paralysis. When you’re ready to work together, let’s get on a call. Book here ↓
Leg Three: Medicine Has No Mechanism for Letting You Change
We change. But our surgical careers don’t.
Back in 1976, Douglas Hall, the career researcher, described two contrasting career models. One, he called the traditional career. This is the type of career we associate with the Baby Boomers (and earlier generations). It’s the career that starts at IBM after grad school…and then retires from IBM at 65.
In the traditional career, the entity in charge isn’t the person, really. It’s the organization. Loyalty is valued, mobility is low, and the rewards are rising rank and salary.
On the other hand, Hall called the other model the protean career (after the shape-shifting Greek god Proteus). The protean career belongs to the individual. That career prizes psychological success, and tolerates lateral moves between industries in the service of freedom and growth.
Menelaus and Proteus by Giulio Bonasone (source)
Most American professions have shifted away from the traditional career and toward the protean model.
A quick example: A friend and former colleague of mine named Robert worked for five years as the Chief Operating Officer of Mercy Ships, an organization that runs hospital ships. We overlapped for the three years that I was the Chief Medical Officer of the charity.
Robert didn’t start out in hospital ships. He began his career at Nokia. Then, after a while, he moved on to work with a national airline company in the US. From there, he shifted to Mercy Ships.
Mobile phones. To airplanes. To hospital ships.
Nobody who looked at Robert’s CV called him a flight risk. He was doing what any career these days does: when growth opportunities are available elsewhere, we follow them.
Not true of surgeons, though. I’d wager that if you were hiring a surgeon into your practice, and their CV looked like Robert’s, you’d be very hesitant to consider them. Changing careers every three to five years? Definitely a flight risk!
That’s because medicine still operates on the traditional model. We choose our specialty in our mid-twenties, step onto the moving sidewalk of our careers, and are expected to ride it to retirement.
(This is to say nothing of the way surgical culture shames people who consider changing. Take a look at this article from Gordon Dickie who literally argues that older doctors should not retire!)
As Danielle Ofri wrote in 2019, the business of medicine is built on the assumption that doctors will always show up, day in and day out, like Janet did.
We will do the right thing for their patients, even when it costs us everything.
The Wellness Trap (and why it doesn’t work for surgeon burnout)
And that, finally, brings me back to resilience training.
It doesn’t work.
That’s not just my opinion either. Over half the studies on physician wellness programs do not show a significant benefit.
And that’s because telling a burned-out physician to breathe more deeply blames the victim for a system that won’t bend. You cannot yoga your way out of a system that’s been built on your back.
Wellness programs, resilience training, and meditation apps fail to move the needle on surgeon burnout because they’re treating the wrong thing.
Burnout in surgery is not a wellness problem. It’s not a resilience problem. It is, instead, the predictable collision of three forces: an identity formed before adulthood, a self that keeps changing, and a profession that pretends that neither of those things is true.
You can’t deep breathe your way out of this three-legged stool.
The only way out is to change the stool you’re sitting on.
Burnout Coaching for Surgeons: A Different Way Forward
If this resonates, then let me remind you: You’re not burnt out because you are weak. You’re burnt out because you’ve been trying to solve a structural problem with personal effort.
Burnout coaching is not about helping you tolerate more. It’s not about getting your mindset right. It’s not about breathing better. It is about helping you see clearly what is actually happening in your life and your work, and then making deliberate choices from that place to get you to a life you’re in love with again.
In our work together, we look at identity, values, workload, and all the myriad (and confusing) factors you’re trying to solve for. We make space for the fact that you have changed, even if your career has not. And we build a path forward that does not require you to abandon everything, but also does not ask you to keep paying the same price. The goal is alignment, so that the life you are living actually fits the person you have become.
It’s about building a life you don’t want to quit.
Feeling burnt out?
You don’t have to navigate it alone. Work with a decision coach who knows how to guide you to a life you’re madly in love with again.
→ Check out my packages here. They range from 4 weeks to a year, and they take you from “what the heck do I do next?” all the way to clarity and a step-by-step plan that honors both your calling and your right to thrive. Click here to apply!
→ Want more FREE weekly content about making consequential life choices with confidence and clarity? Join my mailing list!
FAQs About Burnout in Surgeons
-
Because the acute crisis passed, but the underlying structure did not change. You are still working in the same system, just without the adrenaline that once masked the strain.
-
Yes. In fact, that is often when it hits hardest. Caring deeply is what keeps you showing up, even when the cost to you keeps rising.
Only aligning a career with your deepest values sometimes increases the risk of burnout. This is why burnout coaching focuses on the interplay of all the goals you’re trying to accomplish with your life
-
It is more than normal. It is predictable. You made decisions early in life that your current self may no longer fully agree with.
-
They can help at the margins, but they do not address the root issue. The problem is not your coping skills. It is the mismatch between who you are now and the system you are working in. Wellness programs are a band-aid that work mostly to take the edge off the pain, and keep you coming into clinic day in, day out.
-
Not necessarily. Some people do leave, but many find ways to reshape their careers so they better reflect who they are now.
-
It helps you step out of autopilot. You get clarity on what is driving your burnout, and you begin to make intentional decisions about your work, your identity, and your future.